Overview
Diagnosis of Aplastic Anemia
To diagnose aplastic anemia, your healthcare professional may perform the following tests:
-
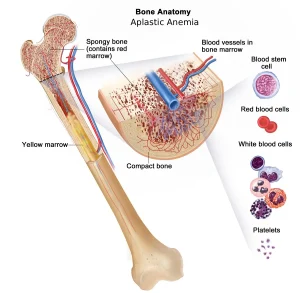
Blood tests: In aplastic anemia, levels of red blood cells, white blood cells, and platelets are lower than normal.
-
Bone marrow biopsy: A needle is used to remove a small sample of bone marrow—usually from the hipbone—for examination under a microscope. In aplastic anemia, the bone marrow shows fewer blood cells than normal.
-
Bone marrow aspiration: A thin needle removes a small amount of liquid bone marrow from the back of the hipbone. This may be done together with a bone biopsy.
Once a diagnosis is confirmed, additional tests may be needed to determine the underlying cause.
Treatment of Aplastic Anemia
Treatment depends on the severity of the disease, symptoms, age, and overall health. Options may include observation, transfusions, medications, or bone marrow transplantation. Severe cases may require immediate hospitalization.
Blood Transfusions
Although not a cure, blood transfusions can temporarily provide blood cells that your bone marrow is not producing. This helps relieve symptoms and prevent complications.
-
Red blood cells: Increase red cell count to ease anemia and fatigue.
-
Platelets: Reduce the risk of excessive bleeding.
Possible complications:
-
Iron overload from repeated transfusions can damage organs. Medicines can remove excess iron.
-
Antibody formation can make future transfusions less effective. Immunosuppressive therapy can help prevent this.
Stem Cell Transplant
A stem cell transplant (bone marrow transplant) may be the only curative option for severe aplastic anemia, especially in younger patients with a matched donor.
Steps of the procedure:
-
Diseased marrow is destroyed with radiation or chemotherapy.
-
Healthy stem cells from the donor are filtered and injected into your bloodstream.
-
The cells migrate to the marrow cavities and produce new blood cells.
🏥 This requires a hospital stay, and medications are given to prevent rejection.
Risks:
-
Transplant rejection
-
Life-threatening complications
-
Not all patients are suitable candidates or have matching donors.
Immunosuppressants
If transplantation isn’t possible, immunosuppressive therapy can help.
-
Common drugs: cyclosporine (Neoral, Sandimmune), antithymocyte globulin, and corticosteroids (methylprednisolone).
-
These medicines suppress immune cells damaging the bone marrow, allowing recovery and new blood cell production.
These drugs can weaken the immune system and relapse may occur after discontinuation.
Bone Marrow Stimulants
Growth factors or colony-stimulating factors can stimulate bone marrow to produce more blood cells.
-
Examples: sargramostim (Leukine), filgrastim (Neupogen), pegfilgrastim (Neulasta), epoetin alfa (Epogen/Procrit), eltrombopag (Promacta).
-
Often used along with immunosuppressants to boost blood cell production.
Antibiotics and Antivirals
Because aplastic anemia weakens immunity, infections can become serious quickly.
-
Early treatment of fever or infection is crucial.
-
Doctors may prescribe antibiotics or antivirals to help prevent or treat infections.
Other Treatments
-
Aplastic anemia caused by radiation or chemotherapy often improves after treatment stops.
-
In pregnancy-related aplastic anemia, symptoms may resolve after childbirth. If not, treatment is required.
Advertisement
