Overview
Diagnosis
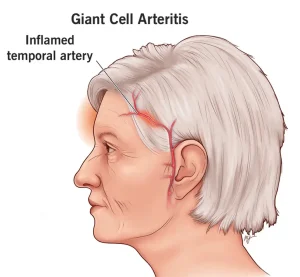
Giant cell arteritis can be challenging to diagnose because its early symptoms are similar to those of other common conditions. To make an accurate diagnosis, your doctor will review your medical history, discuss your symptoms, and perform a detailed physical exam, paying special attention to your temporal arteries. These arteries may feel tender, have a reduced pulse, or appear hard and cordlike.
Blood tests
Blood tests help identify inflammation and monitor how well treatment is working. Common tests include:
-
Erythrocyte sedimentation rate (ESR): Measures how quickly red blood cells settle at the bottom of a test tube. A faster rate can indicate inflammation.
-
C-reactive protein (CRP): Detects levels of a protein produced by the liver during inflammation.
Imaging tests
Imaging studies can help diagnose giant cell arteritis and track your response to therapy. These may include:
-
Doppler ultrasound: Uses sound waves to show blood flow through the arteries.
-
Magnetic resonance angiography (MRA): Combines MRI imaging with contrast dye to produce detailed images of blood vessels.
-
Positron emission tomography (PET): Helps identify inflammation in larger arteries, such as the aorta, using a small amount of radioactive tracer.
Biopsy
A temporal artery biopsy is the most reliable way to confirm giant cell arteritis.
-
The procedure involves removing a small tissue sample from the temporal artery near the scalp.
-
It is performed under local anesthesia and typically causes minimal discomfort.
-
The sample is examined under a microscope for inflammation and the presence of giant cells.
Sometimes, even if giant cell arteritis is present, the biopsy may be negative. In such cases, your doctor may recommend a biopsy on the other side of your head.
Treatment
The main treatment for giant cell arteritis is high-dose corticosteroids such as prednisone. Because untreated giant cell arteritis can cause vision loss, treatment usually begins immediately — even before the diagnosis is confirmed by biopsy.
Corticosteroid therapy
-
Symptoms typically improve within days of starting treatment.
-
If vision loss occurred before treatment began, recovery is unlikely, though your other eye may compensate.
-
Medication may be needed for one to two years or longer, with the dose gradually reduced over time.
-
Headaches or other symptoms can return during the tapering phase, requiring a temporary increase in dosage.
Additional treatments
-
Some people develop symptoms of polymyalgia rheumatica during treatment, which can be managed with a slight increase in corticosteroids.
-
Your doctor may prescribe methotrexate (Trexall) to help suppress the immune system and reduce inflammation.
-
Because long-term corticosteroid use can lead to side effects like osteoporosis, high blood pressure, and muscle weakness, your doctor may recommend calcium and vitamin D supplements or medications to protect bone health.
Newer therapy
The FDA has approved tocilizumab (Actemra) for treating giant cell arteritis. It is given as an injection under the skin and can reduce the need for corticosteroids. However, it may increase the risk of infection, and further research is ongoing to better understand its long-term safety and effectiveness.
Advertisement
