Overview
Diagnosis
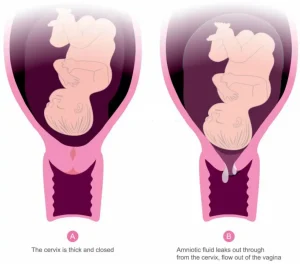
To diagnose preterm labor, your healthcare professional reviews your medical history, risk factors for preterm birth, and current symptoms. If you have regular uterine contractions and your cervix begins to soften, thin, and open before 37 weeks of pregnancy, you may be in preterm labor.
Several tests and procedures are used to confirm the diagnosis and assess risk:
-
Pelvic exam to check how firm or tender the uterus is and to see whether the cervix has started to open. This exam is usually done if the water has not broken and there is no concern about placenta previa. The exam can also help identify uterine bleeding.
-
Ultrasound, most often a transvaginal ultrasound, to measure the length of the cervix. Ultrasound imaging can also show the baby’s size and position, evaluate the placenta, and measure the amount of amniotic fluid.
-
Uterine monitoring to track how long contractions last and how frequently they occur.
-
Lab tests, which may include a vaginal swab to check for infections and to look for fetal fibronectin, a substance released during labor. A urine sample may also be taken to check for bacteria. Test results are reviewed along with other risk factors.
Treatment
If you are at risk of preterm labor, your healthcare team may recommend treatments aimed at reducing the chance that labor will begin too early.
Surgical procedure
A treatment called cervical cerclage involves stitching the cervix closed with strong sutures. This procedure is most often used for people who are less than 24 weeks pregnant, have a history of early premature birth, and have a cervix that is opening or measuring less than 25 millimeters in length. The sutures are usually removed around 36 weeks of pregnancy, or earlier if needed.
Vaginal progesterone
For women found to have a short cervix before 24 weeks of pregnancy, progesterone placed in the vagina may help lower the risk of preterm birth.
Treatments once labor begins
Once preterm labor has started, medicines or surgery generally cannot stop it permanently. However, certain medications may be used to delay delivery briefly or reduce risks to the baby:
-
Corticosteroids, which help lower the risk of complications in babies born prematurely. These include lung problems, bleeding in the brain, severe infection, and death. They are usually recommended if delivery is likely within the next one to seven days and pregnancy is less than 37 weeks.
-
Magnesium sulfate, which may be offered if delivery is expected between 24 and 32 weeks of pregnancy. Some studies show it can reduce the risk of cerebral palsy in babies born before 32 weeks.
-
Tocolytics, medicines that may slow uterine contractions for up to 48 hours. This short delay allows time for corticosteroids to take effect or for transfer to a hospital equipped to care for premature babies.
Tocolytics do not treat the underlying cause of preterm labor and do not improve long-term outcomes for the baby. They are not used if certain conditions are present, such as pregnancy-related high blood pressure or preeclampsia.
If you are at risk of preterm labor and not hospitalized, your healthcare team may ask you to come in weekly or more often so symptoms can be monitored closely.
Advertisement
