Overview
Diagnosis
Hyperthyroidism is diagnosed through a combination of medical history, physical examination, and blood tests. Based on your results, your healthcare provider may recommend additional tests to determine the underlying cause.
Medical history and physical exam
During the exam, your healthcare provider may check for:
-
Slight tremor in the fingers and hands
-
Overactive reflexes
-
Rapid or irregular heartbeat
-
Eye changes such as bulging or irritation
-
Warm, moist skin
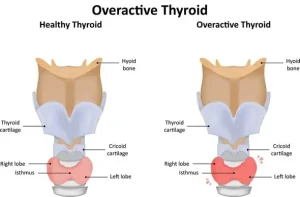
Your provider will also examine your thyroid gland as you swallow to determine if it is enlarged, irregular, or tender.
Blood tests
Blood tests measure thyroid hormones T-4 and T-3 and thyroid-stimulating hormone (TSH). A high T-4 level and a low TSH level typically confirm hyperthyroidism. Blood testing is especially important for older adults who may not show classic symptoms.
Biotin supplements can interfere with thyroid test results. If you take biotin or multivitamins containing biotin, your healthcare provider may ask you to stop taking them for 3 to 5 days before testing to ensure accurate results.
Additional tests
If blood tests confirm hyperthyroidism, further testing can help identify the cause:
-
Radioiodine scan and uptake test: This test measures how much radioactive iodine your thyroid absorbs. High uptake suggests Graves’ disease or overactive thyroid nodules, while low uptake may indicate thyroiditis.
-
Thyroid ultrasound: Uses sound waves to create detailed images of the thyroid and is especially useful for detecting nodules. This test is safe during pregnancy and breastfeeding, as it does not involve radiation exposure.
Treatment
Treatment for hyperthyroidism depends on the underlying cause, your age, overall health, and the severity of the condition. Options may include medications, radioactive therapy, or surgery.
Anti-thyroid medicine
Medications such as methimazole and propylthiouracil reduce hormone production and gradually relieve symptoms within weeks to months. Treatment usually lasts 12 to 18 months. If thyroid levels stabilize, the dose may be reduced or discontinued.
-
Some individuals achieve long-term remission, while others may experience a return of symptoms.
-
Rare side effects include liver damage, rashes, fever, or joint pain. Propylthiouracil is generally reserved for people who cannot take methimazole.
Beta blockers
These medications help manage symptoms such as tremors, rapid heart rate, and palpitations but do not affect hormone levels. They are often used temporarily until hormone levels normalize. Beta blockers are not recommended for people with asthma and may cause fatigue or sexual side effects.
Radioiodine therapy
Radioiodine is taken orally and absorbed by the thyroid gland, gradually shrinking it and reducing hormone production. Symptoms typically improve within several months. This treatment often leads to hypothyroidism, requiring lifelong thyroid hormone replacement with levothyroxine.
Thyroidectomy
Surgical removal of part or all of the thyroid gland is less common but may be recommended for pregnant individuals, those unable to tolerate medications, or those who do not wish to undergo radioiodine therapy.
-
Risks include injury to the vocal cords and parathyroid glands, which regulate calcium levels.
-
After surgery, lifelong thyroid hormone replacement therapy is required. If parathyroid glands are removed or damaged, calcium supplements may also be necessary.
Thyroid eye disease
Thyroid eye disease often accompanies Graves’ disease. Mild cases can be managed with self-care measures such as using artificial tears, lubricating eye gels, and avoiding bright light or wind exposure.
More severe cases may require medications:
-
Corticosteroids (methylprednisolone, prednisone): Reduce swelling behind the eyes.
-
Teprotumumab (Tepezza): Helps control moderate to severe symptoms.
-
Other treatment options include tocilizumab (Actemra), rituximab (Rituxan), and mycophenolate mofetil (Cellcept).
Surgical options for thyroid eye disease:
-
Orbital decompression surgery: Removes bone between the eye socket and sinuses to relieve pressure and improve vision. Risks include persistent or new double vision.
-
Eye muscle surgery: Corrects double vision caused by scar tissue by repositioning affected eye muscles.
With proper diagnosis and treatment, hyperthyroidism and its related complications can be effectively managed, helping restore hormonal balance and overall well-being.
Request an appointment
Advertisement
