Overview
Diagnosis
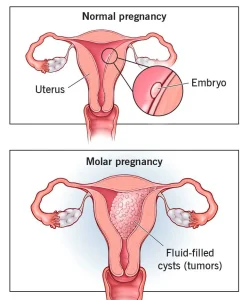
When a molar pregnancy is suspected, a health care provider typically orders blood tests and an ultrasound. During early pregnancy, the ultrasound may be done using a wandlike device placed in the vagina, called a transvaginal ultrasound. By eight or nine weeks of pregnancy, an ultrasound of a complete molar pregnancy may show no embryo or fetus, no amniotic fluid, a thick cystic placenta that nearly fills the uterus or ovarian cysts.
A partial molar pregnancy may appear differently, showing a fetus that is smaller than expected, low amniotic fluid and a placenta with an unusual appearance. After confirming a molar pregnancy, the provider may also check for medical conditions such as preeclampsia, hyperthyroidism or anemia.
Treatment
A molar pregnancy cannot continue because of the risk of complications. The abnormal placental tissue must be removed, and treatment may include one or more steps depending on the situation.
• Dilation and curettage, also called D&C, removes the molar tissue from the uterus. The cervix is opened and the tissue is removed with suction. This is usually performed in a hospital or surgery center with medication to numb the area or help you sleep.
• Removal of the uterus may be considered rarely if there is a high risk of gestational trophoblastic neoplasia and no desire for future pregnancies.
• HCG monitoring is done after treatment to ensure hormone levels return to normal. A continued high level of HCG may require additional treatment.
After treatment, HCG levels are monitored for about six months to confirm no molar tissue remains. If GTN is diagnosed and chemotherapy is needed, monitoring continues for one year after treatment is completed. Because HCG levels rise during a normal pregnancy, a health care provider may recommend waiting 6 to 12 months before trying to conceive again and can help select a reliable form of birth control during this period.
Advertisement
