Overview
Diagnosis
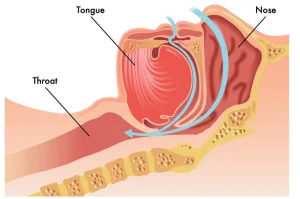
Diagnosis of pediatric obstructive sleep apnea begins with a review of your child’s symptoms and health history, followed by a physical exam. The healthcare professional often examines your child’s head, neck, nose, mouth, and tongue to identify potential causes of airway obstruction.
The main test for pediatric sleep apnea is a polysomnogram, an overnight sleep study. During this test, sensors are placed on your child’s body to record:
• Brain waves
• Breathing patterns
• Snoring
• Oxygen levels
• Heart rate
• Muscle activity
This test is usually performed at a specialized sleep center to provide detailed information about your child’s sleep and breathing.
Treatment
Treatment for pediatric obstructive sleep apnea depends on the severity of the condition, your child’s symptoms, and any underlying risk factors. The primary treatment is often surgery to remove enlarged tonsils and adenoids, known as adenotonsillectomy.
Some children may improve with other approaches, while a few children with mild to moderate sleep apnea may outgrow the condition. In such cases, a healthcare professional may recommend watchful waiting for up to six months, sometimes combined with treatments for allergies or other airway irritants.
Medications
Medications may help relieve mild symptoms of obstructive sleep apnea in children:
• Topical nasal steroids, such as fluticasone or budesonide, can reduce inflammation in the airway
• Montelukast may be used for children with allergies, alone or alongside nasal steroids
Therapies
Devices may be recommended if medications or surgery do not fully resolve sleep apnea:
• Positive airway pressure therapy, including continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BPAP), uses a mask to deliver air pressure and keep the airway open
• Proper fitting and periodic adjustments of the mask ensure comfort as the child grows
• Oral appliances, such as dental devices or mouthpieces, can expand the roof of the mouth, move the jaw or tongue forward, and help keep the airway open; only some children benefit from these devices
Surgery or other procedures
Adenotonsillectomy to remove the tonsils and adenoids is often recommended for children with moderate to severe obstructive sleep apnea.
Other forms of upper airway surgery may be suggested based on your child’s individual condition. Referral to a pediatric ear, nose, and throat specialist is usually needed to discuss surgical options and determine the best approach.
Advertisement
