Overview
Diagnosis
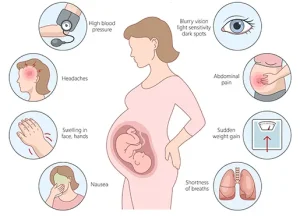
Preeclampsia is diagnosed when high blood pressure develops after 20 weeks of pregnancy along with at least one additional specific finding. These findings indicate that organs such as the kidneys, liver, blood, brain, or lungs may be affected.
A diagnosis is made when high blood pressure is present along with one or more of the following:
-
Protein in the urine, which suggests impaired kidney function
-
Other signs of kidney problems
-
A low blood platelet count
-
Elevated liver enzymes that indicate liver impairment
-
Fluid buildup in the lungs
-
New headaches that do not improve with pain medication
-
New changes in vision
High blood pressure is measured using two numbers. The first number reflects systolic pressure, which is the pressure when the heart is contracting. The second number reflects diastolic pressure, which is the pressure when the heart is resting between beats.
During pregnancy, high blood pressure is diagnosed when the systolic pressure is 140 millimeters of mercury or higher or the diastolic pressure is 90 millimeters of mercury or higher. If a high reading is recorded during an appointment, a second measurement is usually taken at least four hours later to confirm the diagnosis.
Additional tests
If high blood pressure is detected, additional tests are done to look for other signs of preeclampsia and to monitor the health of both the mother and the baby.
These tests may include:
-
Blood tests
Blood samples are analyzed to check how well the liver and kidneys are functioning and to measure platelet levels, which are important for blood clotting. -
Urine analysis
A single urine sample or a 24-hour urine collection is used to assess kidney function and measure protein levels. -
Fetal ultrasound
Ultrasound exams are used to closely monitor the baby’s growth. These images help estimate the baby’s weight and measure the amount of amniotic fluid in the uterus. -
Nonstress test or biophysical profile
A nonstress test checks how the baby’s heart rate responds to movement. A biophysical profile uses ultrasound to assess breathing, movement, muscle tone, and amniotic fluid levels.
Treatment
The main treatment for preeclampsia is either delivering the baby or carefully managing the condition until it is safest to proceed with delivery. This decision depends on how severe the preeclampsia is, how far along the pregnancy is, and the overall health of both the mother and the baby.
If preeclampsia is mild, frequent healthcare visits are usually recommended. Blood pressure, symptoms, and the baby’s well-being are closely monitored. Daily blood pressure checks at home may also be advised.
Treatment of severe preeclampsia
Severe preeclampsia typically requires hospitalization so that blood pressure and potential complications can be closely monitored. The baby’s growth and overall health are also watched carefully during this time.
Medications commonly used for severe preeclampsia include:
-
Drugs to lower blood pressure
-
Anticonvulsant medication, such as magnesium sulfate, to prevent seizures
-
Corticosteroids to help speed up the development of the baby’s lungs before delivery
Delivery
When preeclampsia is not severe, delivery may be recommended after 37 weeks of pregnancy. In cases of severe preeclampsia, delivery is often recommended before 37 weeks, depending on how serious the complications are and how ready the baby is for birth.
The choice between vaginal delivery and cesarean delivery depends on disease severity, the baby’s gestational age, and other medical factors discussed with the healthcare provider.
After delivery
Close monitoring continues after the baby is born because high blood pressure and other symptoms of preeclampsia can persist or develop after delivery. Before leaving the hospital, patients are given clear instructions on when to seek medical care for signs of postpartum preeclampsia, such as severe headaches, vision changes, intense abdominal pain, nausea, or vomiting.
Advertisement
