Overview
Diagnosis
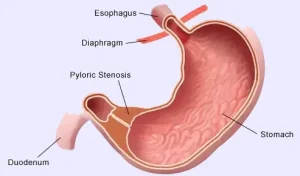
To diagnose pyloric stenosis, a healthcare professional asks about symptoms and performs a physical exam. In some babies, an olive-shaped lump may be felt in the upper belly. This lump represents the enlarged pyloric muscle and is more likely to be detected in later stages of the condition. Wavelike stomach contractions may also be seen during the exam, especially after feeding or just before vomiting.
Imaging tests are often needed to confirm the diagnosis or rule out other causes of vomiting.
Ultrasound
Ultrasound is the primary test used to diagnose pyloric stenosis. A device is moved over the baby’s belly to create images. The test can clearly show thickening of the pyloric muscle.
X-ray
A specialized X-ray study may be used in some cases. The baby drinks a special liquid that shows up on X-ray, allowing the healthcare professional to watch how the stomach fills and empties. This test is done less often than ultrasound.
Blood tests
Blood tests may be done to check for dehydration or imbalances in electrolytes, which are common when vomiting is severe.
Treatment
Surgery is required to treat pyloric stenosis. Before surgery, fluids and electrolytes are given through a vein to correct dehydration and restore balance. This preparation typically takes 24 to 48 hours.
The surgical procedure is called pyloromyotomy. The surgeon makes a cut in the thickened pyloric muscle and spreads it apart down to the stomach lining. This loosens the muscle, allowing food to pass out of the stomach more easily. The muscle still works normally, and the stomach lining bulges into the opening without leaking stomach contents.
Most pyloromyotomy procedures are done using laparoscopic surgery. This method uses three small openings in the belly, one for a camera and two for surgical tools. Some babies may need open surgery through a larger incision, although laparoscopic surgery usually allows quicker recovery.
After surgery, babies are monitored for at least 24 hours. Feeding typically begins 12 to 24 hours after the procedure, either on demand or on a schedule depending on the care team’s plan. Some vomiting can still occur during recovery. Follow-up visits focus on checking the baby’s weight, growth and overall development. Complications such as bleeding or infection are rare, and most babies recover well.
A nonsurgical treatment option may occasionally be considered for babies who are at very high risk for surgery. A medicine called atropine sulfate may help relax the pyloric muscle. However, this approach is less effective than surgery and generally requires a longer hospital stay.
Advertisement
