Overview
Diagnosis
Several tests may be used to diagnose solitary rectal ulcer syndrome, depending on symptoms and clinical findings. These tests help evaluate rectal structure, bowel function and muscle coordination.
Sigmoidoscopy
This test uses a thin, flexible tube with a camera to examine the rectum and part of the colon. If a lesion is seen, a tissue sample may be collected for further laboratory testing through a biopsy.
Anorectal manometry
Anorectal manometry evaluates how well the bowel functions. A flexible tube is placed into the rectum to measure the response of the anal and rectal muscles and nerves. It is often used to assess constipation, fecal incontinence and other disorders involving stool control.
Defecography
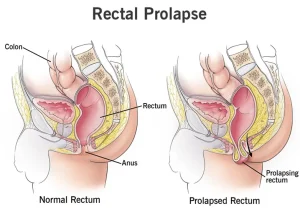
During defecography, a soft barium paste is inserted into the rectum. You then pass the barium during imaging. The barium appears clearly on X-rays and may help identify a rectal prolapse or issues involving muscle function and coordination. Some medical centers offer magnetic resonance defecography using an MRI machine for a more detailed, 3D view of the rectum.
Ultrasound
Ultrasound uses sound waves to create internal images and may help differentiate solitary rectal ulcer syndrome from other conditions with similar symptoms.
Treatment
Treatment for solitary rectal ulcer syndrome depends on symptom severity. Mild cases may improve with lifestyle adjustments, while more severe cases may require medical or surgical treatment.
Dietary changes
Increasing fiber intake can help improve constipation and reduce straining during bowel movements.
Behavior therapy
Some people strain out of habit when passing stool. Behavior therapy helps retrain pelvic muscles and encourages relaxation during bowel movements. Biofeedback is often included in this approach, teaching you how to control involuntary body responses, such as tightening of the anus or pelvic floor muscles. This can make you more aware of straining and help you reduce it.
Medicines
Certain medical treatments may help relieve symptoms. Options can include topical steroids, sulfasalazine enemas, onabotulinumtoxinA injections or argon plasma coagulation. These treatments may not work for everyone, and some are still considered experimental.
Surgical procedures
Surgery may be recommended for people with severe symptoms or when other treatments have not provided relief.
• Rectal prolapse surgery, also known as rectopexy, may be suggested if a prolapse is contributing to symptoms. This procedure secures the rectum in its correct position.
• Surgery to remove the rectum may be considered for severe cases that do not respond to other therapies. The surgeon may create an opening in the abdomen for waste to exit the body, called a colostomy. A pouch is then attached to collect waste.
Advertisement
