Overview
Diagnosis
Trigeminal neuralgia is diagnosed primarily based on your description of the pain. Key factors include:
• Type – Sudden, brief, electric shock-like pain.
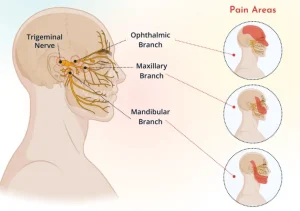
• Location – The areas of the face affected indicate which branch of the trigeminal nerve may be involved.
• Triggers – Pain may be triggered by eating, talking, light facial touch, or even a cool breeze.
Healthcare professionals may conduct tests to confirm the diagnosis and rule out other causes:
• Neurological exam – Evaluates facial sensation, reflexes, and identifies affected nerve branches.
• Magnetic resonance imaging (MRI) – Checks for underlying causes such as multiple sclerosis or tumors. A contrast dye may be used to visualize blood vessels and blood flow.
Other tests may be performed if needed to exclude other conditions that can mimic trigeminal neuralgia.
Treatment
Treatment of trigeminal neuralgia usually starts with medications. Some people respond well to medication alone, while others may need injections or surgery if medications are ineffective or cause side effects. If trigeminal neuralgia is caused by another condition, such as multiple sclerosis, treatment of the underlying cause is necessary.
Medications
Medicines help reduce or block pain signals sent to the brain:
• Anti-seizure medicines – Carbamazepine is commonly prescribed. Others include oxcarbazepine, lamotrigine, phenytoin, topiramate, pregabalin, and gabapentin. Doses may be adjusted if effectiveness decreases. Side effects can include dizziness, confusion, drowsiness, and nausea. Genetic testing may be recommended before carbamazepine in certain populations.
• Muscle relaxants – Baclofen may be used alone or with anti-seizure medicines to reduce pain and muscle tension. Side effects may include drowsiness, nausea, and confusion.
• Botox injections – OnabotulinumtoxinA injections may relieve pain in some people when medications are insufficient. Research is ongoing.
Surgical options
Surgical procedures may be considered when medications are not effective:
• Microvascular decompression – Moves or cushions blood vessels pressing on the trigeminal nerve. Can provide long-term pain relief, but carries risks such as hearing loss, facial weakness, numbness, or stroke.
• Brain stereotactic radiosurgery (Gamma Knife) – Focused radiation targets the trigeminal nerve root to reduce pain. Relief may take up to a month and may need to be repeated if pain returns. Facial numbness is a common side effect.
Other procedures include rhizotomy techniques that damage nerve fibers to block pain:
• Glycerol injection – Injected into the nerve to block pain signals. May cause facial numbness; pain may return in some cases.
• Balloon compression – Inflates a balloon to damage part of the nerve and reduce pain. Usually causes temporary facial numbness.
• Radiofrequency thermal lesioning – Uses heat to destroy nerve fibers associated with pain. Some temporary facial numbness is expected, and pain may recur after several years.
Treatment choice depends on symptom severity, patient health, and response to prior therapies. Regular follow-up is essential to manage recurrence and monitor side effects.
Advertisement
